Pericardial effusion estimation is usually done cualitatively. Measurements of systolic and diastolic
dimensions from parasternal in M-mode is important, in order to allow follow-up controls. Hemodynamic
severity can be assessed through evidence of atrial or ventricular wall compression, interventricular
septum displacement during inspiration and inferior vena cava plethora with blunted respiratory response.
Left:
small pericardial effusion with inferior basal localization.
Right:
small pericardial effusion with posterior basal localization.
Left:
circular, mid-size pericar- dial effusion, with posterior und lateral accentuation.
Right:
mid-size pericardial effu- sion, as well as large pleural effusion clear delimitated
through parietal pericardial line.
Left:
mid-size to large pericardial effusion with severe hemodynamic compromise,
as evidenced through RV compression.
Right:
large, circular pericardial effusion. RV and LV filling show respiratory dependent compro- mise.
Left:
this same case from the parasternal short axis. Aspirated volumen was 1.5 liters.
Right:
inferior vena cava is plethoric and without respiratory collapse, a sign of hemodynamic
severity.
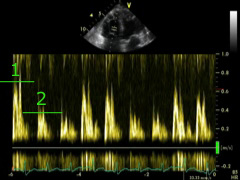
Following images show charac- teristics of pericardial compres- sion.
Left:
contraction of the free RV wall is impeded through the organized pericardial effusion. RV
expands during filling at the beginning of each inspiration, only through a septal shift toward
the LV (septal bounce).
Right:
E-wave shows a clear (> 25 %) increase in inspiration (1).
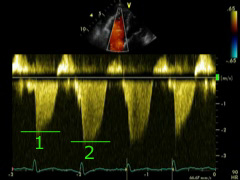
Left:
tricuspid regurgitation is also more evident during inspiration, here more accentuated
as in physiologic status.
Right:
tricuspid regurgitation maximal velocity becomes lower as EROA increases.
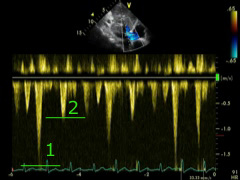
Left:
inferior vena cava is plethoric and show no inspiratory collapse.
Right:
antegrade velocities in suprahepatic vein also show clear respiratory accentuacion.

 ORC
ORC