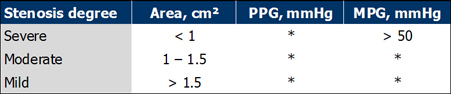
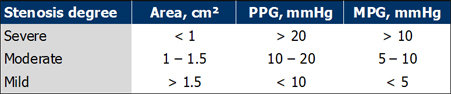
* information not available (Bonow et al. Circulation 1998;98:1949-1984)
PPG = peak pressure gradient, MPG = mean pressure gradient
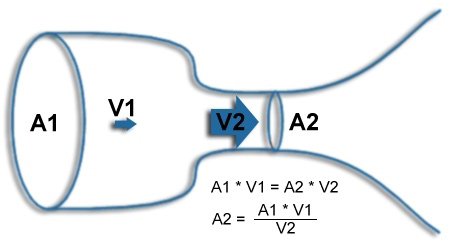
2. Continuity equation:
standard method to calculate valvular opening area. Systolic velocities in left
ventricular outflow track (LVOT) and on the aortic valve, as well
as LVOT area must be assessed.
A2 = aortic stenosis area, V2 = aortic stenosis velocity time integral (VTI, obtained with CW-Doppler),
A1 = LVOT area and V1 = LVOT VTI (obtained with PW-Doppler).
Calculation of the continuity equation can be usually made in every echomachine, but in case this is not
possible, hier an
online
calculator of the Canadian Society of Echocardiography.
Pitfalls in the assessment of a severe aortic stenosis are: the low-output low-gradient aortic stenosis
and the pinhole stenosis. In case of the presence of morphologic criteria for severe aortic stenosis
(thickened aortic valve with important decrease of leaflets separation, severe left ventricular
hypertrophy) examination ends first after assessment of maximal velocities from standard views,
as well as from the subcostal, suprasternal and right parasternal views.
The examination of a relevant aortic valve stenosis is considered incomplete, if maximal velocities are
not documented form the right parasternal view (patient lies on the right side).
A transesophageal examination should be considered in difficult cases, maximal velocities can
be obtained here from the transgastric five-chamber view.
Left:
assessment of valvular morphology ist the first step to a correct diagnosis of
valvular heart disease. Here a cross sectional view of the aortic valve from
the parasternal short axis view.
Right:
the aortic valve is thickened, calcified and with severely reduced leaflet separa- tion,
as seen from the apical five-chamber view.
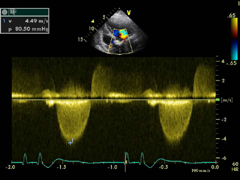
Left:
color Doppler helps to CW-Doppler beam positioning. Pin hole stenoses are very difficult to
examine, fact that can lead to important underestimation of velocities.
Right:
maximal velocities from 4.5 m/s or above (peak pressure gradient aprox. 80 mmHg) can be considered
as a thumb rule for severe aortic stenosis.
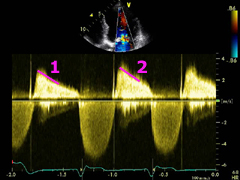
Correct assessment of the pressure half time (PHT) is decisive for calculating
mitral valvular opening area, correspondingly its stenosis degree. This can be difficult in
case of atrial fibrillation, since Doppler profile inclination varies with the
duration of diastole.
Left:
a dilated left atrium is a common occurrence to a signi- ficant mitral stenosis.
Right:
the degree of thickness, calcification and movement limitation of the whole mitral valve
apparatus are important parameters for decision to a percutaneous valvuloplasty
(Wilkins-Score, online
calculator from the Canadian Society of Echocardiography).
Left:
a concurrent mitral valve regurgitation must be included in the evaluation before
valvulo- plasty.
Right:
different values of PHT can be obtained in case of atrial fibrillation, according to
diastole length. It is importante to find a mean value, that correlate to measured
values of transmitral gradients.
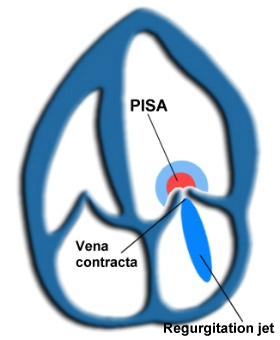
All valvular regurgitations have three components: PISA (proximal isovelocity surface area),
vena contracta and regurgitation jet. PISA can be spontaneously seen when regurgitation is
already significant. Vena contracta plays a more important role for assessment of degree
of regurgitation than regurgitation jet.
A vena contracta with an area larger than 50 % of LVOT, with a regurgitation jet deceleration >3 m/s²
and a diastolic retrograde flow in the descendant aorta can be consistent with the diagnosis of
a severe aortic regurgitation.
A wide vena contracta with a v-shaped regurgitation jet (CW-Doppler), PISA and systolic retrograde flow
into the pulmonary veins can be consistent with the diagnosis of a severe mitral regurgitation. A TEE
examination to exclude e.g. partial ruptured chordae tendineae can be necessary in this case,
especially in presence of an eccentric mitral regurgitation.
A retrograde flow into the hepatic veins together with the afore mentioned parameters lead to
the diagnosis of a severe tricuspid regurgitation.
2. Parameters for quantitative assessment: EROA,
regurgitation volumen, regurgitation fraction
New "high-end" echomachines simplify the assessment of the effective
regurgitation orifice area (EROA), regurgitation volume and fraction.
Assessment of EROA can be carried out with the continuity equation, where A1 (PISA area),
V1 (PISA Nyquist-limit) and V2 (regurgitation VTI) are the known variables, and A2
(EROA) the variable to be calculated.
EROA = (PISA area x PISA Nyquist-limit) / regurgitation VTI
Regurgitation volume = SVreg - SVnorm
SVreg: Stroke volume measured at the regurgitating valve
SVnorm: Stroke volume measured at a valve without regurgitation
Calculations with the PISA method can usually be made directly in the echomachine, alternatively
here an
online
calculator from the Canadian Society of Echocardiography. Excentric regurgitations may produce
inaccurate results.
Left:
color Doppler settings must be correctly adjusted for the PISA method. The Nyquist-limit should
be placed around 50-60 cm/s.
Right:
afterwards, base line should be shifted in the direction of the regurgitation jet,
until a well-defined hemisphere appears.
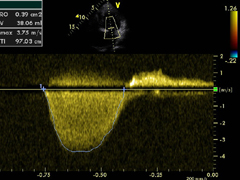
Left:
to calculate VTI of regurgi- tation jet, CW-Doppler profile area should
be delineated.
Right:
by measuring PISA radius it is important to hit correctly the limit ot the hemisphere.
Small errors can produce important variations.
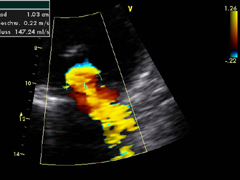
Left:
furthermore, it is very im- portant to define the cause of the valvular regurgitation.
Here a TEE examination of partial ruptured chordae tendineae of the posterior mitral
leaflet.
Right:
a severe, excentric mitral regurgitation can be verified with color Doppler.
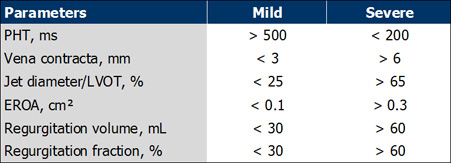
The following morphofunctional parameters of severe aortic regurgitation are in part historic,
in part very much up-to-date. Most of them can be documented in a (standard) routine examination,
only a few demand additional especial views and machine settings.
In case of suspicion of a sever aortic regurgitation, the examiner has the task to observe and
document them, as well as to derive the corresponding interpretation. The echocardiography report
can help on the decision about the urgency of an invasive examination and the subsequent surgical
correction. A comprehensive assessment of valve morphology can be achieved with a TEE examination.
2D-Echo
1. Significant annuloaortic ectasia with incomplete coaptation of aortic cusps
2. Prolaps of one (or more) aortic cusp/s (with or without dissection of the aortic root)
3. Aortic cusp perforation
4. LVEDD > 60 mm (> 35 mm/m²)
5. LVESD > 50 mm (> 25 mm/m²)
6."Reversed doming" of the anterior mitral leaflet
7. Dilated left atrium
8. Strong pulsating aortic arch (suprasternal view)
9. Strong pulsating abdominal aorta (subxyphoid view)
M-Mode
10. Premature mitral valve closure
11. High frecuency diastolic vibration of the anterior mitral leaflet
12. High frecuency diastolic vibration of the interventricular septum
Color Doppler
13. Vena contracta > 6 mm
14. Regurgitation jet > 50 % of LVOT diameter or LVOT surface (short axis view)
15. Coanda effekt
16. Extremely short jet, as braked in LVOT
CW Doppler
17. High density of regurgitation envelope
18. Steep decline of regurgitation envelope profile
19. PHT < 200 ms
20. Deceleration of regurgitation profile > 3m/s²
PISA (color and CW Doppler)
21. EROA > 0,4 cm²
22. Regurgitation volumen > 60 mL
PW Doppler
23. Diastolic flow reversal in the descending aorta (suprasternal view) > 25% of the diastole
24. Diastolic flow reversal in the abdominal aorta (subxyphoid view)
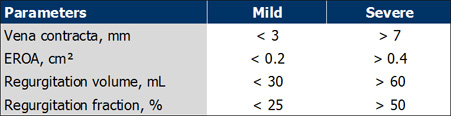
The following morphofunctional parameters of severe mitral regurgitation can be documented in a
(standard) routine examination, only a few demand additional especial views and machine settings.
In case of suspicion of a sever aortic regurgitation, the examiner has the task to observe and
document them, as well as to derive the corresponding interpretation. The echocardiography report
can help on the decision about the urgency of an invasive examination and the subsequent surgical
correction. A comprehensive assessment of valve morphology can be achieved with a TEE examination.
2D-Echo
1. Dilated mitral annulus with incomplete valvular coaptation
2. Mitral valve prolapse or leaflet segment prolapse (with or without rupture of chordae tendineae)
3. Papillary muscle dysfunction (with or without rupture)
4. Mitral leaflet perforation
5. Functional classification Carpentier type IIIb
6. Dilated LA
7. LVEDD > 60 mm (> 35 mm/m²)
8. LVESD > 35 mm (> 20 mm/m²)
Color Doppler
9. Vena contracta > 7 mm
10. Coanda effect
11. Extremely short jet, as braked in LA
CW Doppler
12. High density of regurgitation envelope
13. "V-Wave cutoff" sign
14. Slow systolic peak velocities (e.g. 4 m/s)
PISA (Color and CW Doppler)
15. EROA > 0,3 cm²
16. Regurgitation volumen > 60 mL

 ORC
ORC